Gum disease is not just a mouth problem and it does not go away on its own.
What every Estonian should know about periodontitis, inflammation, and their health. The story of one patient and a very common situation.
Today I received a letter from Southern Estonia. A 59-year-old person visited the periodontology department of Tartu University Hospital at the beginning of the year. An X-ray was taken, a 3D examination was conducted. The next appointment: in three months, in May. No treatment was prescribed or performed.
When asked about the role of vitamin D, the specialist replied: "Gum diseases are not treated with vitamin D." But the tooth is moving. It hurts. The patient feels inflammation and a bad taste in the mouth. The letter ended with a question that stuck with me: "I don't know how and where to go next; the inflammation is worsening."
In the past year, this person has already had three teeth removed. This is not an isolated case. It is a system. I would like to talk more about the statement "Gum diseases are not treated with vitamin D" today, as this statement is a half-truth that turns into injustice.
What is periodontitis actually?
Periodontitis, or colloquially gum disease, is not merely a "gum problem".
It is a chronic bacterial-immune inflammatory disease that destroys the bone and connective tissue surrounding the teeth.
The disease usually starts quietly. There is bleeding in the gums, slight swelling, an unpleasant odor. Many people ignore it for years, and dentists often treat the symptom (tartar removal), not the cause.
As the disease progresses, periodontal pockets form, cavities between the tooth and the gum where anaerobic bacteria accumulate. There is a lack of oxygen, antibiotics do not penetrate well, and the body's immune response paradoxically begins to harm itself by destroying bone to "extinguish" the infection.
The result: the tooth begins to move.
Important: chronic periodontitis does not heal on its own. Without treatment, it always progresses.
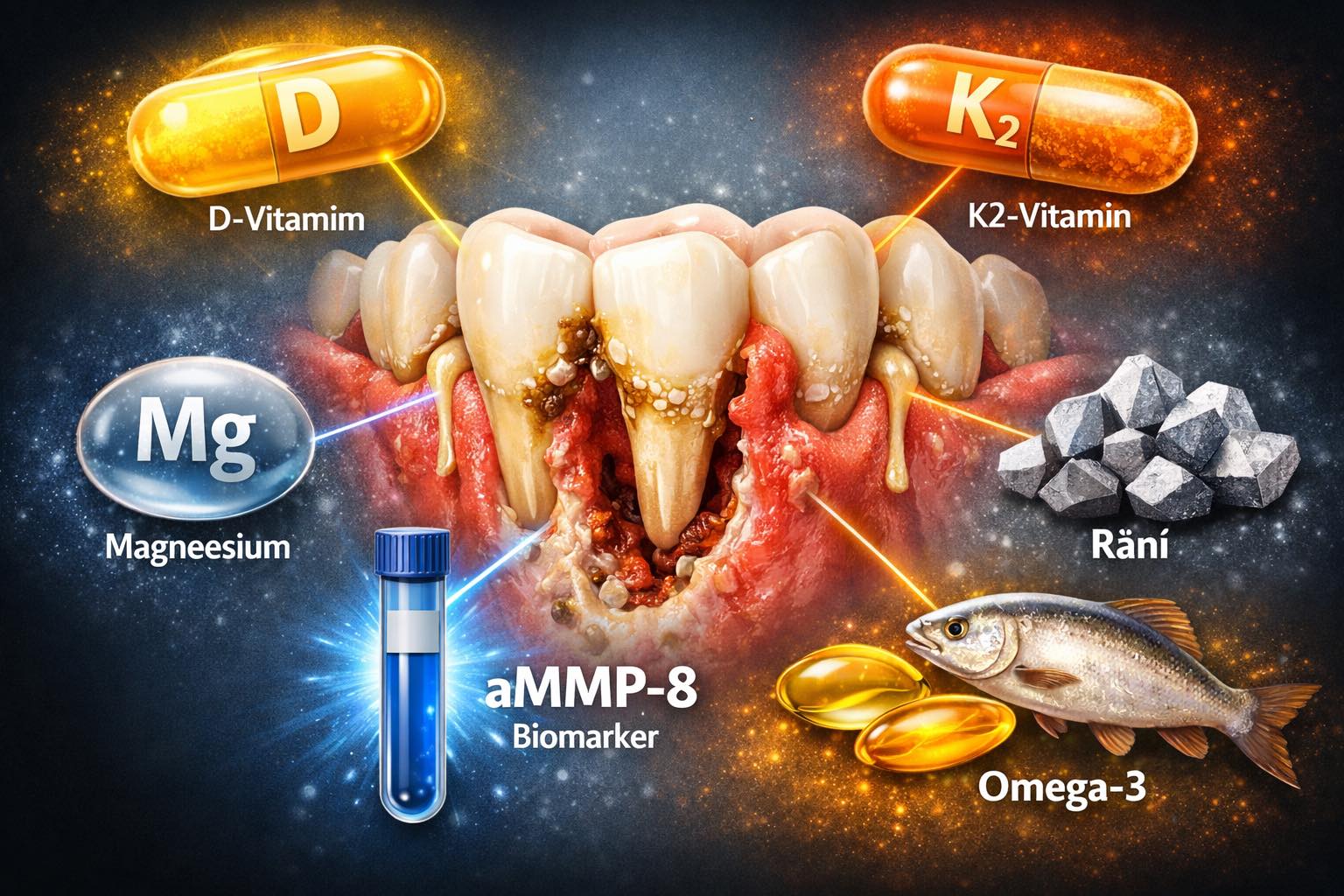
aMMP-8: a biomarker that is hardly used in Estonia.
One question you should ask your dentist: "Do you measure the aMMP-8 level?"
aMMP-8 (activated matrix metalloproteinase-8) is an enzyme released by neutrophils during active inflammation. It breaks down collagen, the very collagen that keeps the tooth's connecting tissue together.
The largest research groups in the world (Prof. Timo Sorsa, Helsinki) have shown that the aMMP-8 level in oral fluid precedes clinically visible bone loss by 6–12 months. This means that before bone loss occurs, we can already prevent it, meaning we can detect the disease before irreversible damage is done.
What measuring aMMP-8 allows:
• To detect hidden active inflammation even when the patient does not feel pain
• To monitor the effectiveness of treatment with objective numbers (not just "I feel better")
• To give the patient a clear signal: "your inflammation is active, you need immediate treatment"
The aMMP-8 saliva test is the first-level diagnostic tool in the Fullgevity protocol.
Vitamin D and gum disease, what does science actually say?
Now back to this statement: "Gum diseases are not treated with vitamin D."
Technically, this is true. Vitamin D does not clean periodontal pockets, does not remove biofilm, does not replace mechanical cleaning (SRP).
But to say that vitamin D has no connection to gum disease is clinically misleading.
Here’s what studies show:
• Vitamin D directly regulates the immune response, affecting the activity of T-cells, macrophages, and neutrophils. A low level of vitamin D means a dysregulated inflammatory response. Usually, greater problems occur for those whose level is below 75nmol/L.
• Vitamin D receptors (VDR) are present in periodontal tissues, and its deficiency is associated with a more severe form of periodontitis (Machado et al., 2021, Journal of Periodontology).
• Vitamin D affects calcium absorption and bone metabolism, specifically the bones that periodontitis destroys.
• An optimal level of vitamin D (70–100 nmol/L) is associated with a lower progression of periodontitis.
Clinical message: Vitamin D does not cure periodontitis. But its deficiency makes the disease worse and the treatment less effective. This is an important difference.
Vitamin K2 and magnesium as forgotten allies.
Vitamin D does not work in isolation. Two of its key partners are vitamin K2 and magnesium.
Vitamin K2 (menaquinone-7): directs calcium into bones and teeth, not into soft tissue. Without K2, high vitamin D paradoxically may increase arterial calcification. K2 activates the osteocalcin protein, which helps maintain the alveolar (bone around the tooth) bone.
Magnesium: involved in over 300 enzymatic reactions as a cofactor. It enzymatically activates vitamin D. Without magnesium, vitamin D does not convert to active calcitriol. Additionally, magnesium regulates inflammatory cytokines (IL-6, TNF-α) and is linked to insulin sensitivity.
Practical recommendation: When taking vitamin D, also check magnesium and K2 levels.
Optimal combination: D3 + K2 (MK-7) + magnesium bisglycinate.
Omega-3 is not just a "heart medication"
Omega-3 fatty acids (EPA and DHA) have two roles that are often not mentioned in periodontology:
1. Resolution of inflammation, not just suppression.
The body synthesizes resolving molecules and protectins from omega-3s, which actively end the inflammatory process. This is fundamentally different from the inflammation suppression based on aspirin or ibuprofen. Chronic inflammation is characterized by a lack of resolution capability; the body cannot finish it.
2. Omega-3 index as a mirror of systemic inflammation.
An omega-3 index (EPA+DHA in erythrocytes) below 4% is associated with higher cardiovascular risk, higher SII (systemic immune inflammation index), and increasing research shows a connection to more severe periodontitis as well.
Fullgevity routinely tests the omega-3 index alongside aMMP-8 and vitamin D — these three form our inflammatory biomarker basic panel.
What is evidence-based standard and what should a patient demand?
EFP (European Federation of Periodontology) 2022 treatment guidelines are clear:
1. For stage II–IV periodontitis, mechanical subgingival debridement (SRP — scaling and root planing) must be started as soon as possible.
2. The patient must be educated about oral hygiene and monitored before the next appointment.
3. In the case of active inflammation, a three-month treatment gap is not sufficient.
4. Systemic factors (vitamin D, supplements and medications, diabetes, general illnesses, blood tests, smoking, stress) must be included in treatment planning and tactics.
What can and should a patient ask:
→ "What stage of periodontitis do I have (I–IV)?"
→ "When does mechanical treatment start — not just diagnostics?"
→ "Is aMMP-8 or any other inflammatory biomarker being measured?"
→ "Have my vitamin D, omega-3, and magnesium levels been checked?"
→ "What is my SII and SIRI level?"
→ "Can I use Lumoral, cranberry mouthwash, etc.?"
Summary: five things you need to know
1. Periodontitis does not go away on its own. It progresses quietly, often painlessly, until there are no teeth left.
2. Biomarkers inform before teeth move. aMMP-8 detects active inflammation before irreversible bone loss.
3. Vitamin D, K2, and magnesium do not cure periodontitis — but their deficiency makes the disease harder to treat. Optimal levels support the immune response and bone regeneration.
4. Omega-3 is not just for the heart. It helps end chronic inflammation, not just suppress it.
5. Your oral health affects your heart, blood glucose, brain. Periodontitis is a systemic disease. Treat it systemically.
If you have questions about your gum health, biomarker tests, or a second opinion, please write to us. Fullgevity's goal is to connect oral health diagnostics with systemic health image.