To anesthetize or not?
Why do I not recommend treating teeth under anesthesia and what does it really mean for you? I have been practicing dentistry for over 35 years. My patients know that I almost never use anesthesia when treating cavities. Anesthesia is a wonderful thing. But it is also... a mask.
If a tooth reacts during treatment, it is a signal and a "stop" notification. The body says, "hey, you are going too deep" or "you are touching something you shouldn't touch." Under anesthesia, this signal is not heard. If the doctor ignores it, a tooth sensitivity, root canal treatment, potential tooth fracture, or filling dislodgement is soon to come.
I want to hear this feeling because it helps me work more precisely and gently - more biologically.
But why is this important at all?
The biggest mistake in modern dentistry is that too much is done, too quickly, too extensively, too early, and too expensively. Every tooth that is drilled weakens slightly and gets traumatized. Each time more is removed than necessary, the tooth loses something that cannot be returned. Living and regenerating protective tissue is lost, the bond of the filling with the tooth tissue weakens, and the risk of pulp damage increases.
Dentin, the layer beneath enamel, is not just a base for fillings. It is living tissue. There are nerve endings, fluid, its own defense system. If it is excessively removed, the protection is lost. Sensitivity arises. There is a risk of pulp damage. And after some time, the same tooth will need more extensive treatment than was initially necessary.
Biological dentistry means a different philosophy.
Not: "we drill until all tooth tissue is hard."
But: "we understand what is alive and what is not, and we preserve everything that can be preserved."
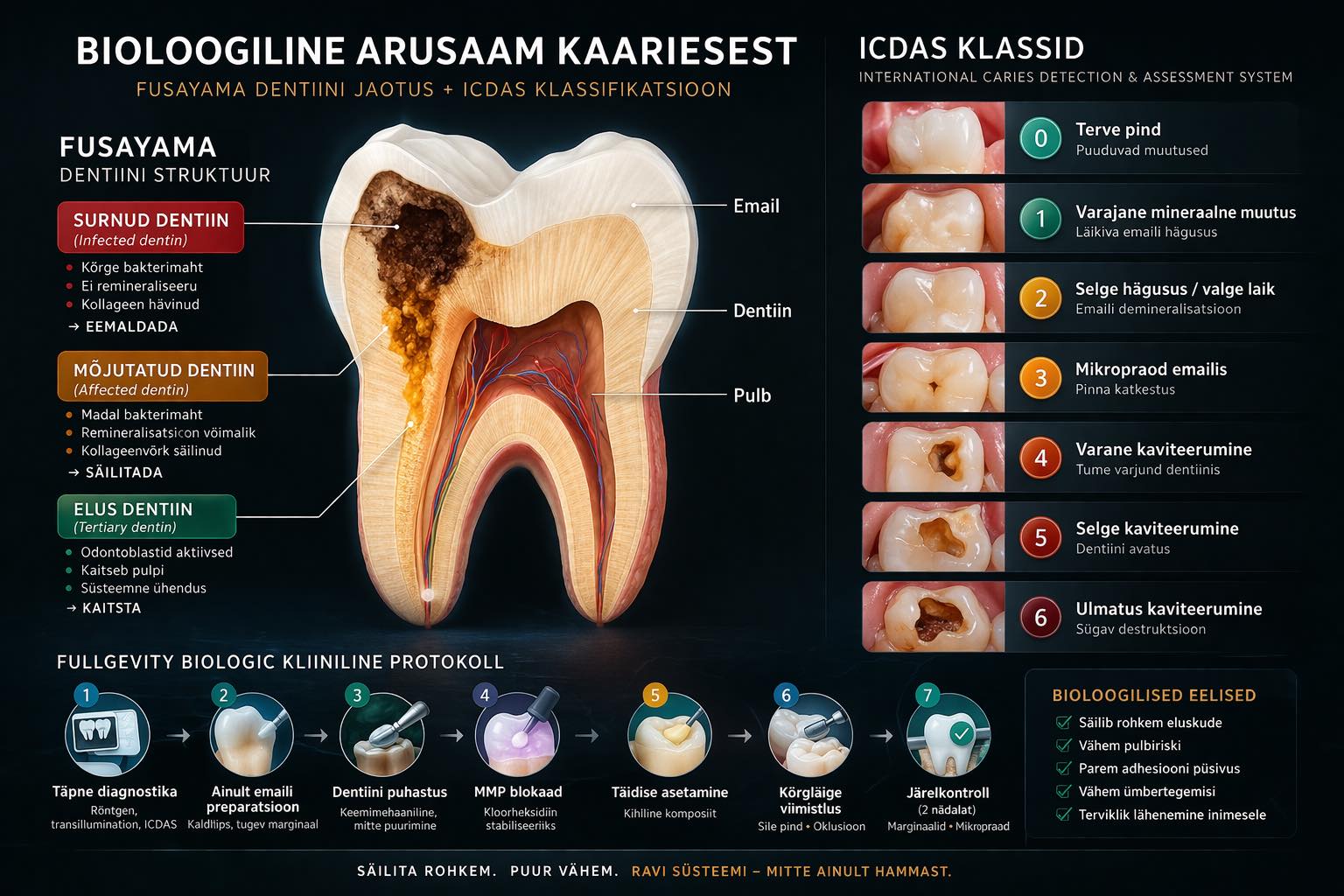
Damaged dentin is removed; that part is dead and painless. Living dentin, even the softer layer that is still intact, is left untouched. This is called selective removal. This is Biological biology.
What to ask your dentist before treatment?
Here are three questions that will give you a good picture of the philosophy with which the doctor sits in front of you.
First: "Do you use anesthesia for cavity treatment?" If the answer is "yes!" then you are already aware for what's ahead.
Second: "Do you use selective atraumatic chemomechanical removal for cavities?" A good answer is "yes." If the doctor does not know what you are talking about, then that also says something.
Third: "How much do you preserve versus remove?" A good dentist should be able to explain what they preserve and why. If the answer is "I remove all soft until I get to hard," then that is an old model. The new model asks: is this soft layer still alive? If it is, it stays put.
Additionally, it's worth asking: "Is treatment needed right now or can we monitor it first?"
Many cavities do not require drilling. Early-stage damage is treatable without drilling and filling. This can be done through dietary changes, biofilm management, and remineralization.
If the doctor immediately says, "it needs to be treated," then ask: "what stage is the damage in?" You have the right to know.
Anesthesia is not inherently bad. But if every treatment goes under anesthesia, it's worth asking: "why?" Has the tooth hurt so much? Or is the treatment so invasive that the body otherwise wouldn't allow it? A dentist who answers these questions clearly and calmly is a dentist worth trusting.
With a modest, unhurried cavity treatment, you can avoid root canal treatment and implants.
Look carefully at the accompanying picture; there are 2 detailed explanations.
If you have questions about your teeth, send a message. I will speak honestly.
Dr. Meeme Luks
Fullgevity Dental, Tallinn